Sun Laboratory
Duxin Sun, PhD
Dr. Duxin Sun is Associate Dean for Research and the Charles Walgreen Jr. Professor of Pharmacy and Pharmaceutical Sciences at the University of Michigan College of Pharmacy. He is the founding director of the Institute of AI-Driven Therapeutics Discovery and also directs the Pharmacokinetics (PK) Core. He holds joint appointments in the Chemical Biology program, the Interdisciplinary Medicinal Chemistry program, and the University of Michigan Comprehensive Cancer Center.
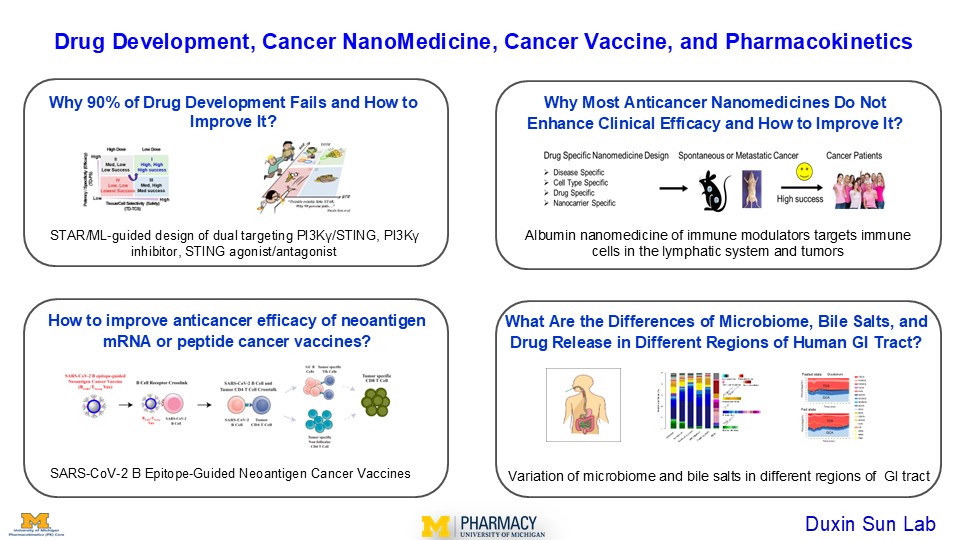
Dr. Sun’s research focuses on drug development, cancer nanomedicine, cancer vaccines, and pharmacokinetics. He established the STAR system (Structure–Tissue/Cell Selectivity–Activity Relationship) to address the 90% failure rate in drug development. He has designed albumin-based nanomedicines that improve the efficacy of immuno-oncology drugs by targeting immune cells in the lymphatic system and tumors, and developed SARS-CoV-2 B epitope–guided neoantigen peptide and mRNA vaccines that activate CD4/CD8 T cell immunity through B cell–mediated antigen presentation.
Dr. Sun holds a BS in Pharmacy, an MS in Pharmacology, and a PhD in Pharmaceutical Sciences, with additional training in molecular biology as a visiting scientist. Drawing on research experience in both academia and industry, he has published more than 300 papers and mentored 40 PhD students and 75 postdoctoral fellows and visiting scientists. An elected Fellow of the American Association for the Advancement of Science (AAAS) and the American Association of Pharmaceutical Scientists (AAPS), he has served on the FDA Pharmaceutical Science and Clinical Pharmacology Advisory Committee and on NIH and FDA study sections.
Dr. Sun’s administrative Specialist is Erika Zucal – [email protected].
Lab and Research Overview
- Why does 90% of drug development fail and how improve it?This project aims to improve drug development success and efficiency through STAR-guided design of dual-targeting PI3Kγ/STING agents, PI3Kγ inhibitors, STING agonists/antagonists, and JAK inhibitors for the immunotherapy of cancer and autoimmune disease.The 90% failure rate in drug development has not improved over the past 40 years, despite significant advances at each step of the process. Adding more testing or criteria is impractical, as bringing a single drug to approval already takes 10–15 years and costs $1–2 billion. Current strategies, including AI-driven approaches, risk falling into a “survivorship bias” trap—focusing on peripheral problems while overlooking the root causes of failure.We propose the STAR-guided drug design system (Structure–Tissue/Cell Selectivity–Activity Relationship) to improve both success rate and efficiency by addressing three overlooked, interdependent factors: (a) On-/off-target potency and specificity (PS) and tissue/cell selectivity (TS) in diseased tissues at clinically relevant doses, which determine clinical efficacy; (b) On-/off-target PS and TS in normal organs at clinically relevant doses, which drive adverse effects and on-/off-target toxicity; (c) Optimal clinical doses, defined by both PS and TS, that balance efficacy and safety.
The STAR system prioritizes Class I drugs (high efficacy, high safety, high success rate) over the Class II–IV drugs (low efficacy, low safety, low success rate) that current strategies tend to produce.
Selected publications
Can machine learning overcome the 95% failure rate and reality that only 30% of approved cancer drugs meaningfully extend patient survival? Duxin Sun, Christian Macedonia, Zhigang Chen, Sriram Chandrasekaran, Kayvan Najarian, Simon Zhou7, Tim Cernak, Vicki L. Ellingrod, H.V. Jagadish, Bernard Marini, Manjunath Pai, Angela Violi, Jason C. Rech, Shaomeng Wang, Yan Li1, Brian Athey, Gilbert S. Omenn. J Med Chem, 2024, 67, 16035
Why 90% of Clinical Drug Development Fails and How to Improve It? Duxin Sun, Wei Gao, Hongxiang Hu, Simon Zhou. Acta Pharmaceutic Sinica B, 2022, 12, 3049
Dual targeting of PI3Kγ and STING overcomes regulatory B cell- and myeloid cell-driven immune suppression in pancreatic cancer. Chengyi Li, Fang Ke, Hongyi Zhao, Shuai Mao, Mahamadou Djibo, Linqi Huang, Miao He, Meilin Wang, Hanning Wen, Zhongwei Liu, Zhixin Yu, Zhihong Qi, Ana R. Xavier, Minal Nenwani, Bo Wen, Nicole Peterson, Vaibhav Sahai, Deepak Nagrath, Carrie L. Lucas, Matthias P. Wymann, Wei Gao, Lawrence Fong & Duxin Sun. Nature Cancer, 2026, https://www.nature.com/articles/s43018-026-01158-7
A gastrointestinal (GI) locally-activating Janus Kinae (JAK) inhibitor to treat ulcerative colitis. Yingzi Bu, Mohamed Dit Mady Traore, Luchen Zhang, Lu Wang, Zhongwei Liu, Duxin Sun. J Biol Chem, 2023, 299: 105467
Design of Potent Small-Molecule Stimulator of Interferon Gene Inhibitor and Stimulator of Interferon Gene Mutant-Specific Degrader. Hong-Yi Zhao, Luchen Zhang, Zhongwei Liu, Miao He, Meilin Wang, Qiuxia Li, Farzad Sarkari, Jinsong Tao, Bo Wen, Venkatesha Basrur, Hannah Myatt, Alexey Nesvizhskii, Duxin Sun. J Med Chem, 2025, https://pubs.acs.org/doi/epdf/10.1021/acs.jmedchem.5c00123?ref=article_openPDF
Design of an Oral STING Agonist through Intramolecular Hydrogen Bond Ring Mimicking to Achieve Complete Tumor Regression. Hong-Yi Zhao, Jinsong Tao, Luchen Zhang, Qiuxia Li, Miao He, Bo Wen, Zhongwei Liu, Hannah Myatt, Duxin Sun. J Med Chem, 2025, 68: 11365
- Why do most anticancer nanomedicines fail to enhance clinical efficacy and how to improve it?This project develops albumin-based nanomedicines to enhance the clinical efficacy of immuno-oncology drugs (STING agonists and PI3Kγ inhibitors) by targeting immune cells in the lymphatic system and tumors for cancer immunotherapy.Anticancer nanomedicines are intended to act as biological missiles, targeting tumors to improve efficacy while minimizing toxicity in normal organs. Yet despite outstanding performance in preclinical cancer models, most have failed to demonstrate superior clinical efficacy—fueling a decades-long debate over current nanomedicine design strategies.We propose a drug- and nanocarrier-specific design strategy to improve clinical success by addressing four questions: (a) Cancer-specific: What features of a given cancer type can be exploited for targeted delivery? (b) Cell-specific: Which cell types must the drug reach? (c) Drug-specific: What intrinsic limitations of the drug need to be overcome? (d) Nanocarrier-specific: Which nanocarrier is best suited to overcome those limitations?
Selected publications
What Went Wrong with Anticancer Nanomedicine Design and How to Make It Right. Sun D, Zhou S, Gao W. ACS Nano. 2020 Oct 27;14(10):12281-12290.
Reappraisal of anticancer nanomedicine design criteria in three types of preclinical cancer models for better clinical translation. Luan X, Yuan H, Song Y, Hu H, Wen B, He M, Zhang H, Li Y, Li F, Shu P, Burnett JP, Truchan N, Palmisano M, Pai MP, Zhou S, Gao W, Sun D. Biomaterials. 2021; 275:120910.
Albumin nanoparticle containing a PI3Kγ inhibitor and paclitaxel in combination with α-PD1 induces tumor remission of breast cancer in mice. Yudong Song, Luke Bugada, Ruiting Li, Hongxiang Hu, Luchen Zhang, Chengyi Li, Hebao Yuan, Krishani Rajanayake, Nathan Truchan, Fei Wen, Wei Gao, and Duxin Sun. Science Translational Medicine, 2022, 14, eabl3649
Albumin-Bound STING Agonist Reprograms HSPCs to Antitumor Neutrophils Enhancing CD8+ T Cell Immunity. Jinsong Tao, Hong-Yi Zhao, Chengyi Li, Hanning Wen, Fang Ke, Qiuxia Li, Miao He, Bo Wen, Zhongwei Liu, Kai Sun, Wei Gao, Duxin Sun. Advanced Science, 2026, https://doi.org/10.1002/advs.202523603
Albumin nanocomplex of BCL-2/xL inhibitor reduced platelet toxicity and improved anticancer efficacy in myeloproliferative neoplasm and lymphoma. Hongxiang Hu, Chengyi Li, Yudong Song, Jizhao Xie, Qiuxia Li, Fang Ke, Bo Wen, Shaomeng Wang, Wei Gao, Duxin Sun. Biomaterials, 2025, 322:123347
- How can we improve the anticancer efficacy of neoantigen mRNA and peptide cancer vaccines?This project develops SARS-CoV-2 B epitope–guided neoantigen peptide and mRNA cancer vaccines that enhance anticancer efficacy by activating CD4/CD8 T cell immunity through B cell–mediated antigen presentation.Current neoantigen vaccines rely primarily on dendritic cell– and macrophage-mediated antigen presentation to activate CD4/CD8 T cell antitumor immunity. However, emerging evidence indicates that B cell–mediated antigen presentation also plays a vital role in anticancer immunity, and it remains unknown whether incorporating this pathway into neoantigen vaccines can improve their efficacy. To address this gap, we developed SARS-CoV-2 B epitope–guided peptide and mRNA neoantigen vaccines designed to engage B cell–mediated antigen presentation alongside conventional pathways, thereby more effectively activating CD4/CD8 T cell antitumor immunity in melanoma, pancreatic, and breast cancers.Selected publications
Antigen-Clustered Nanovaccine Achieves Long-Term Tumor Remission by Promoting B/CD 4 T Cell Crosstalk. Chengyi Li, Ryan Clauson, Luke F. Bugada, Bing He, Hongwei Chen, Hongxiang Hu, Polina Chuikov, Ke Fang, Brett D. Hill, Syed M. Rizvi, Yudong Song, Kai Sun, Daniel Huynh, Marilia Cascalho, Lana Garmire, Leo Yu Lei, Irina Grigorova, Fei Wen, Wei Gao, Duxin Sun. ACS Nano 2024, 18: 9584-9604
SARS-CoV-2 B Epitope-Guided Neoantigen NanoVaccines Enhance Tumor-Specific CD4/CD8 T Cell Immunity Through B Cell Antigen Presentation. Chengyi Li, Shuai Mao, Zera Montemayor, Mohamed Dit Mady Traore, Alejandra Duran, Fang Ke, Mahamadou Djibo, Hanning Wen, Wei Gao, Duxin Sun. ACS Nano, 2025, 19, 7038
- How do the microbiome, bile salts, and drug release differ across regions of the human GI tract?This project investigates regional differences in the microbiome, bile salts, and drug release across the human stomach, small intestine, and colon, and examines how these differences affect drug product development and disease states.Optimizing in vitro and in vivo drug release across the gastrointestinal (GI) tract is critical to oral drug development. Bile salt, which shift between fasting and fed states, influence drug release, disease states, and the microbiome, while the GI microbiome itself helps regulate both disease and drug response. To characterize these factors, we directly measured drug release in the stomach, duodenum, jejunum, and ileum for immediate-release, modified-release, and locally acting drug products; profiled 15 bile salts across regions of the small intestine under fasting and fed conditions; and mapped microbiome composition across regions of the small intestine and colon.Selected publications
Spatial and Temporal Analysis of the Stomach and Small-Intestinal Microbiota in Fasted Healthy Humans. Seekatz AM, Schnizlein MK, Koenigsknecht MJ, Baker JR, Hasler WL, Bleske BE, Young VB, Sun D. mSphere. 2019 Mar 13;4(2):e00126-19.
In Vivo Dissolution and Systemic Absorption of Immediate Release Ibuprofen in Human Gastrointestinal Tract under Fed and Fasted Conditions. Koenigsknecht MJ, Baker JR, Wen B, Frances A, Zhang H, Yu A, Zhao T, Tsume Y, Pai MP, Bleske BE, Zhang X, Lionberger R, Lee A, Amidon GL, Hasler WL, Sun D. Mol Pharm. 2017 Dec 4;14(12):4295-4304.
Measurement of in vivo Gastrointestinal Release and Dissolution of Three Locally Acting Mesalamine Formulations in Regions of the Human Gastrointestinal Tract. Yu A, Baker JR, Fioritto AF, Wang Y, Luo R, Li S, Wen B, Bly M, Tsume Y, Koenigsknecht MJ, Zhang X, Lionberger R, Amidon GL, Hasler WL, Sun D. Mol Pharm. 2017 Feb 6;14(2):345-358.
Lab Members

Bo Wen
Associate Research Scientist, Managing Director of PK Core
Fang Ke
Research Investigator

Erika Zucal
Administrative Specialist (Sun Lab and PK Core)

Hanning Wen
Ph.D. Student

Neha Karekar
Ph.D. Student

Hannah Myatt
Ph.D. Student

Lu Wang
Research Lab Specialist (PK Core)

Miao He
Research Lab Specialist (PK Core)

Tuyen Nguyen
Research Fellow

Fanli Shi
Ph.D. Student

Sanduni Premathilaka, PhD
Research Fellow

Merna Sitto
Technician General Intermediate

Xin Guo, PhD.
Visiting Scientist